Is there a correlation of Body Weight and Osteoarthritis?
The joints in our legs bear the weight of our bodies during everyday activities such as walking, standing, running, and climbing. Due to our anatomy, the forces exerted on the joint surfaces of our hips and knees can exceed seven times our body weight. Consequently, the more weight—whether in the form of muscle or fat—we carry, the greater the burden on these critical joints. This increased load is one of the reasons heavier individuals are more likely to require total hip and knee replacements compared to those with a normal body weight, and why the risk of such procedures escalates with additional weight. Maintaining a healthy weight or losing excess weight can alleviate hip and knee pain and may help prevent or postpone the need for joint replacement surgery.
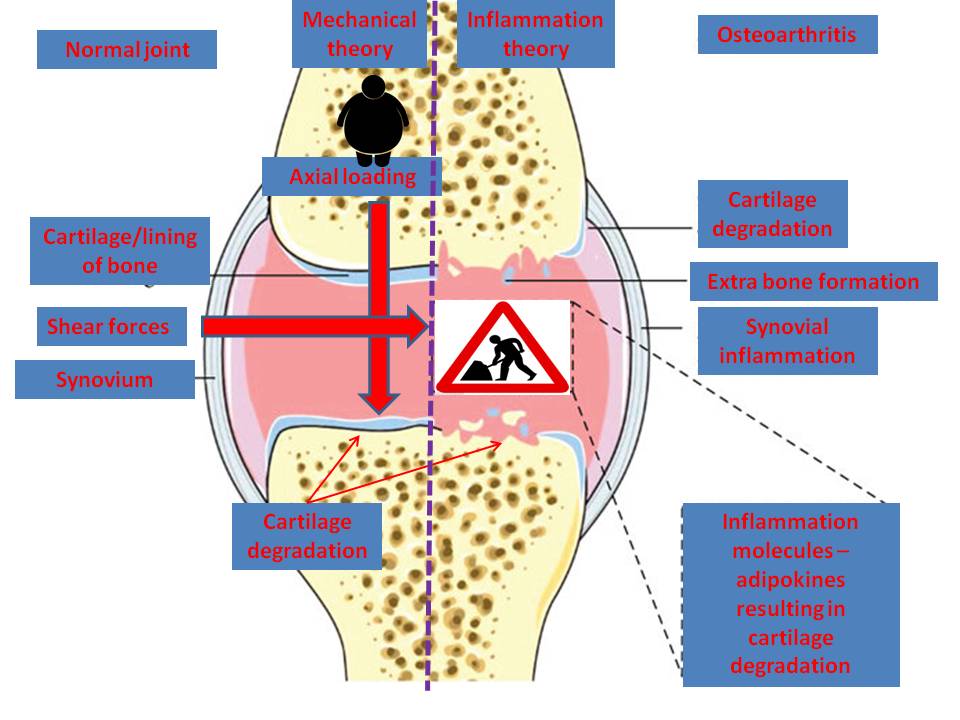
Historically, the link between increased body weight and osteoarthritis has often been attributed to mechanical factors. However, other elements can exacerbate this relationship, such as the overall alignment of the legs, past injuries (like fractures), previous surgeries (such as partial meniscectomies), and pre-existing conditions like rheumatoid arthritis.
Recent research has revealed that adipose (fat) tissue acts as an active and inflammatory organ. It produces numerous factors known as adipokines, which have been linked to the onset of osteoarthritis. In simpler terms, excess body fat can create a state of generalized inflammation, resulting in both metabolic and inflammatory stress.
Moreover, adipokines released by hypertrophic and hyperplastic adipose tissue can activate the NLRP3 inflammasome, leading to systemic inflammation. This response can be intensified during viral infections, which helps explain the severe effects observed in obese individuals infected with SARS-CoV-2, particularly in the context of metabolic and inflammatory stress.
In summary, the correlation between body weight and osteoarthritis is multifaceted, encompassing both mechanical and biological factors. Reducing body weight may serve as a crucial strategy in managing and preventing osteoarthritis, while also highlighting the critical role of fat tissue in overall health and inflammation.
References:
- Chaofan Zhang, et al. Adipokine Signaling Pathways in Osteoarthritis. Front Bioeng Biotechnol. 2022 Apr 19:10:865370. doi: 10.3389/fbioe.2022.865370. eCollection 2022.
- Mobasheri A, Batt M. An update on the pathophysiology of osteoarthritis. Ann Phys Rehabil Med. 2016 Dec;59(5-6):333-339. doi: 10.1016/j.rehab.2016.07.004. Epub 2016 Aug 18. PMID: 27546496.
- Xie, C., Chen, Q. Adipokines: New Therapeutic Target for Osteoarthritis?. Curr Rheumatol Rep 21, 71 (2019).
- Conde J, et al. Adipokines and osteoarthritis: novel molecules involved in the pathogenesis and progression of disease. Arthritis. 2011;2011:203901. doi: 10.1155/2011/203901. Epub 2011 Aug 18. PMID: 22046513; PMCID: PMC3200120.
- Gomez R, et al. Adipokines in the skeleton: influence on cartilage function and joint degenerative diseases. J Mol Endocrinol. 2009 Jul;43(1):11-8. doi: 10.1677/JME-08-0131. Epub 2009 Feb 24. PMID: 19240195.
- Francisco V, et al. Biomechanics, obesity, and osteoarthritis. The role of adipokines: When the levee breaks. J Orthop Res. 2018 Feb;36(2):594-604. doi: 10.1002/jor.23788. Epub 2017 Nov 28. PMID: 29080354.
- López-Reyes A, et al. NLRP3 Inflammasome: The Stormy Link Between Obesity and COVID-19. Front Immunol. 2020 Oct 30;11:570251. doi: 10.3389/fimmu.2020.570251. PMID: 33193349; PMCID: PMC7662564.
- Zapata-Linares N, et al. Role of adipose tissues in osteoarthritis. Curr Opin Rheumatol. 2021 Jan;33(1):84-93. doi: 10.1097/BOR.0000000000000763. PMID: 33186248.
- Carrión M, et al. The Adipokine Network in Rheumatic Joint Diseases. Int J Mol Sci. 2019 Aug 22;20(17):4091. doi: 10.3390/ijms20174091. PMID: 31443349; PMCID: PMC6747092.